tDCS for Depression and Psychiatric Disorders: What Patients Should Know
- Alexander Papp, MD
- Aug 3, 2025
- 5 min read
Updated: Mar 16
Learn how transcranial direct current stimulation (tDCS) works, its role in treating depression and other psychiatric disorders, and how it compares to rTMS as a noninvasive neuromodulation option.
What Is tDCS? A Brief Overview
Transcranial direct current stimulation (tDCS) is a noninvasive neuromodulation technique that delivers a weak, low-intensity electrical current to the brain through two scalp electrodes — an anode and a cathode. Unlike treatments that directly trigger nerve impulses, tDCS works by gently shifting cortical activity. Anodal stimulation is associated with increased neural activity, while cathodal stimulation tends to reduce it. With repeated sessions, these shifts are thought to promote longer-lasting changes in brain plasticity — essentially, helping the brain reorganize and adapt over time.
How Does tDCS Work in the Brain?
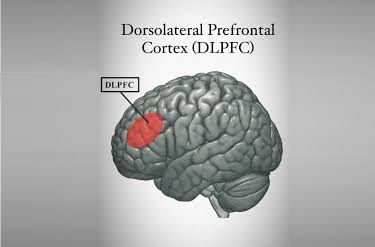
In psychiatric applications, tDCS most commonly targets the dorsolateral prefrontal cortex (DLPFC) — a brain region centrally involved in mood regulation, executive function, and cognitive control. The stimulation is believed to modulate the balance between excitatory and inhibitory nerve activity, and may influence important neurotransmitters including glutamate, GABA, dopamine, and serotonin. Intensities studied in clinical research typically range from 0.5 to 3 milliamps (mA), applied for sessions lasting 20 to 30 minutes. These parameters vary depending on the condition being treated and the electrode placement, known as the montage.
tDCS for Depression: The Strongest Evidence

Among all psychiatric applications, tDCS has the most robust evidence base for depression. Multiple meta-analyses (see e.g. Razza 2020) have found active tDCS to be superior to sham (placebo) stimulation for reducing depressive symptoms. In quantitative terms, one major review reported response rates of approximately 33% with active tDCS versus 17% with sham, and remission rates of roughly 19% versus 10%. Importantly, evidence suggests that tDCS works best as an add-on strategy — that is, combined with antidepressant medication — rather than as a standalone treatment. Evidence-based expert guidelines have rated tDCS as 'definitely effective' for depressive episodes, though it is important to note that it is not currently FDA cleared and remains investigational in standard clinical practice.
tDCS in Schizophrenia and Other Psychiatric Conditions
Beyond depression, researchers have explored tDCS for severel other conditions. In schizophrenia, meta-analyses suggest that tDCS may improve negative symptoms, positive symptoms, and auditory hallucinations. Current VA/DoD clinical guidance has judged the evidence insufficient to recommend tDCS for or against use in schizophrenia at this time but found it promising in PTSD and chronic pain. For OCD and ADHD, early-stage reviews point to possible benefits, but the certainty of evidence remains low and no established clinical guidelines exist for these indications. As with depression, tDCS for these conditions is best understood as investigational.
Safety and Tolerability: What to Expect
One of tDCS's most clinically attractive features is its tolerability profile. The vast majority of reported adverse effects are mild and transient: skin irritation, tingling or burning sensations under the electrodes, mild headache, itchiness, neck discomfort, or slight drowsiness. Serious adverse effects have not been reported in the psychiatric literature. One review did note an increased incidence of abnormally elevated mood in response to tDCS treatment, which is an important consideration particularly when treating patients with bipolar disorder. Overall, tDCS does not appear to cause cognitive side effects, and discontinuation rates in clinical trials are comparable to sham stimulation.
tDCS vs. rTMS: Understanding the Differences
Repetitive transcranial magnetic stimulation (rTMS) and tDCS are both noninvasive brain stimulation modalities, but they differ in evidence, regulatory status, and practical delivery. rTMS has FDA clearance for major depression and is more embedded in standard psychiatric practice, typically administered across 20 to 30 in-clinic sessions over four to six weeks. tDCS, by contrast, remains investigational, though it offers the advantage of simpler, more portable equipment — and home-based protocols have been studied. In head-to-head network meta-analyses of depressive disorders, rTMS generally ranks ahead of tDCS in antidepressant effect size, particularly for treatment-resistant depression and in older adults. That said, both modalities outperform sham for depressive symptom reduction in the broader literature.
Who Is a Good Candidate for tDCS?
Based on current evidence, the patients most likely to benefit from tDCS are adults with non-treatment-resistant unipolar depression, particularly as an adjunct to medication. Adults with bipolar depression who need an additional, well-tolerated augmentation option are another group where tDCS has shown promise in randomized controlled trials — with antidepressant benefit and no clear excess of mood switching compared to sham. tDCS may also be particularly well suited to patients for whom frequent clinic attendance is a significant barrier; home-based tDCS protocols have been explored with encouraging preliminary results, including one study that observed remission in 11 of 20 participants with bipolar depression over a 6-week home protocol.
For patients with more treatment-resistant depression or when maximizing established efficacy is the priority, rTMS carries a stronger evidence base and regulatory standing. The 2023 VA/DoD Bipolar Disorder guidelines also support offering adjunctive rTMS for bipolar depression after inadequate response to pharmacotherapy, a recommendation not yet matched by comparable guidance for tDCS.
Setting Realistic Expectations: Informed Consent and Counseling
Patients should understand the current strength of evidence, the realistic probability of nonresponse, and the practical burdens involved, including session frequency and whether the treatment is available locally. For tDCS specifically, patients should understand that while the evidence is encouraging — particularly for depression as part of a combined treatment approach — it does not yet have the same regulatory standing as some other neuromodulation options. Shared decision-making, grounded in honest expectation-setting, is essential for any patient exploring these interventions.
The Bottom Line on tDCS
Transcranial direct current stimulation represents a promising, lower-intensity form of neuromodulation — particularly for adults with depression who are not highly treatment-resistant and for whom portability or reduced treatment burden matters. Its evidence base in psychiatry is growing, and its tolerability profile is favorable. At the same time, it is best viewed as a complementary option within a broader treatment plan, rather than a first-line or standalone intervention. As the research continues and protocols become more standardized, tDCS may increasingly find its place alongside established neuromodulation tools. Patients interested in tDCS are encouraged to discuss their individual clinical profile with their psychiatrist.
References
Non-invasive cortical stimulation: Transcranial direct current stimulation (tDCS). Sudbrack-Oliveira P, Razza LB, Brunoni AR, International Review Of Neurobiology. 2021
A systematic review and meta-analysis on the effects of transcranial direct current stimulation in depressive episodes. Razza LB, Palumbo P, Moffa AH, et al. Depression And Anxiety. 2020
Neurobiological Mechanisms of Transcranial Direct Current Stimulation for Psychiatric Disorders; Neurophysiological, Chemical, and Anatomical Considerations. Yamada Y, Sumiyoshi T, Frontiers In Human Neuroscience. 2021
Matsumoto H, Ugawa Y. Adverse events of tDCS and tACS: A review. Clin Neurophysiol Pract. 2016 Dec 21;2:19-25.
A systematic review and meta-analysis on the effects of transcranial direct current stimulation in depressive episodes. Razza LB, Palumbo P, Moffa AH, et al., Depression and Anxiety. 2020;37:594–608.
____________________
Alexander Papp, MD


